Deceased Donor Organ Allocation
About this research
The lab studies organ allocation systems for deceased donors, addressing the critical shortage of available organs against high patient demand. The current heart transplant allocation system relies on treatment intensity rather than objective illness severity markers, creating perverse incentives where some transplant centers escalate care to artificially increase patient priority.
Analysis of data from the Scientific Registry of Transplant Recipients found that high-benefit centers prioritize truly sick candidates and maximize lives saved, while low-benefit centers over-treat stable patients. OPTN's 2018 reforms increased status levels from 3 to 6, restricting top priority to cardiogenic shock patients.
Scarce Therapeutics Allocation
About this research
The lab develops evidence-based policies for allocating scarce therapeutic resources, with emphasis on vaccine distribution during COVID-19. Research addresses proactive outreach strategies, place-based allocation approaches, and the potential benefits of delaying second doses to extend initial coverage.
A study of 2.7 million residents found that Non-Hispanic Black residents comprised 80% of the least vaccinated zip codes. Modeling indicated that equal vaccination rates could have prevented 119 Alpha wave deaths and 108 Delta wave deaths. Analysis also identified gaps between the CDC's three ethical principles and actual vaccine allocation policies.
This work has been featured in the New York Times, Washington Post, USA Today, and Chicago Tribune.
Crisis Standards of Care
About this research
Crisis standards of care provide ethical guidance for healthcare systems during public health emergencies. They enable resource prioritization when demand exceeds supply, directing allocation decisions toward patients with highest survival likelihood.
A review found that 92% of 26 state guidelines recommended objective scoring systems for ventilator allocation. Retrospective analysis revealed that while Black and White patients had similar SOFA scores, Black patients demonstrated lower in-hospital mortality at equivalent scores, creating a systemic disadvantage in allocation systems that rely on SOFA-based triage.
The CLIF Consortium standardizes critical care data across 17 institutions and 46 hospitals, enabling large-scale research on equitable allocation and outcomes in intensive care settings.
Published in



Research Spotlights
Featured publications from the lab
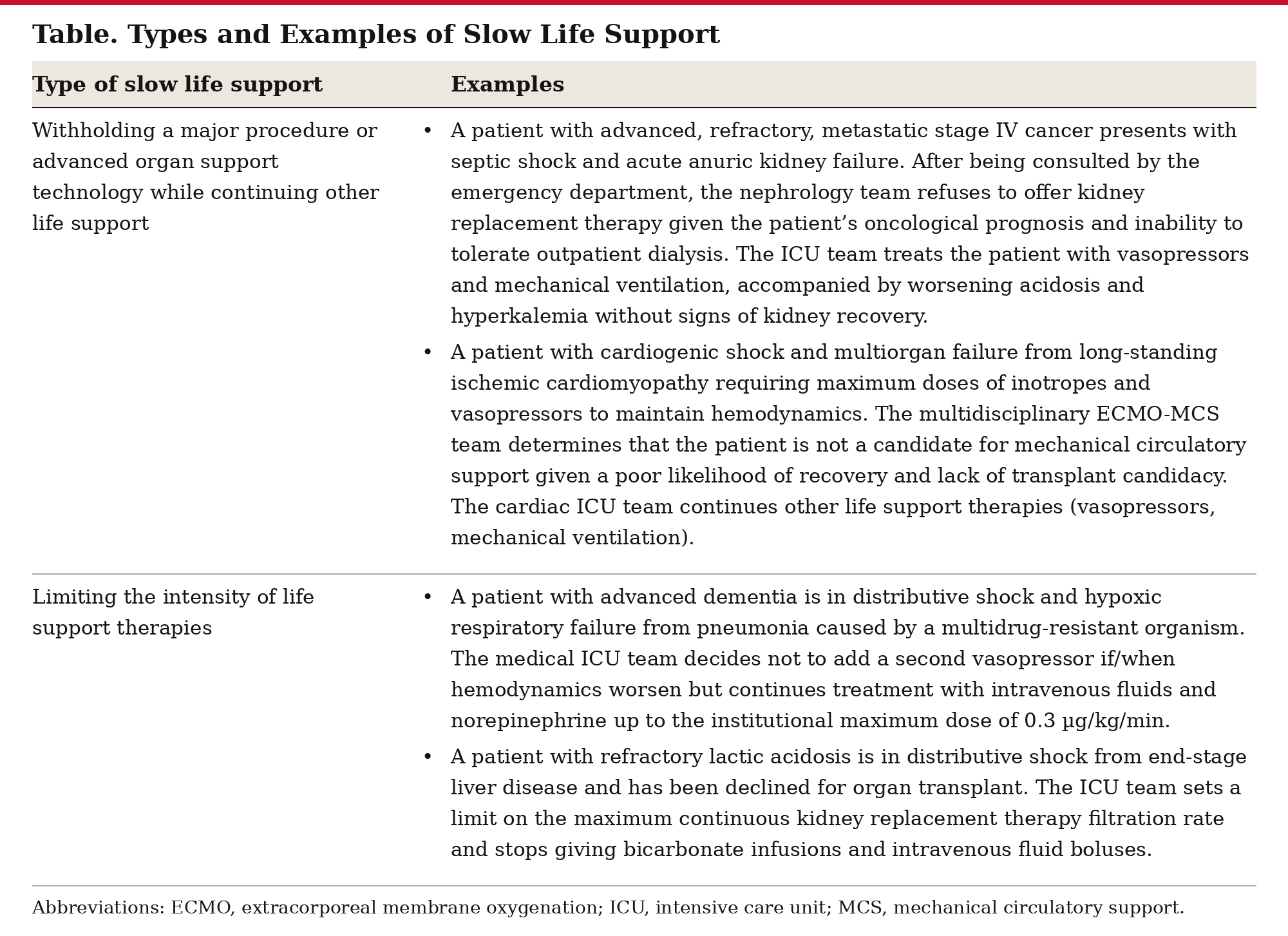

Slow Life Support for Imminently Dying Patients
Beyond communication, the boundaries of unilateral clinician authority must be clarified when initial shared decision-making is unable to negotiate a coherent life support plan. Informed assent, wherein clinicians explicitly disclose a recommended treatment path and its best-case and worst-case potential outcomes to patients or surrogates, may provide the most optimal balance of core ethical principles.
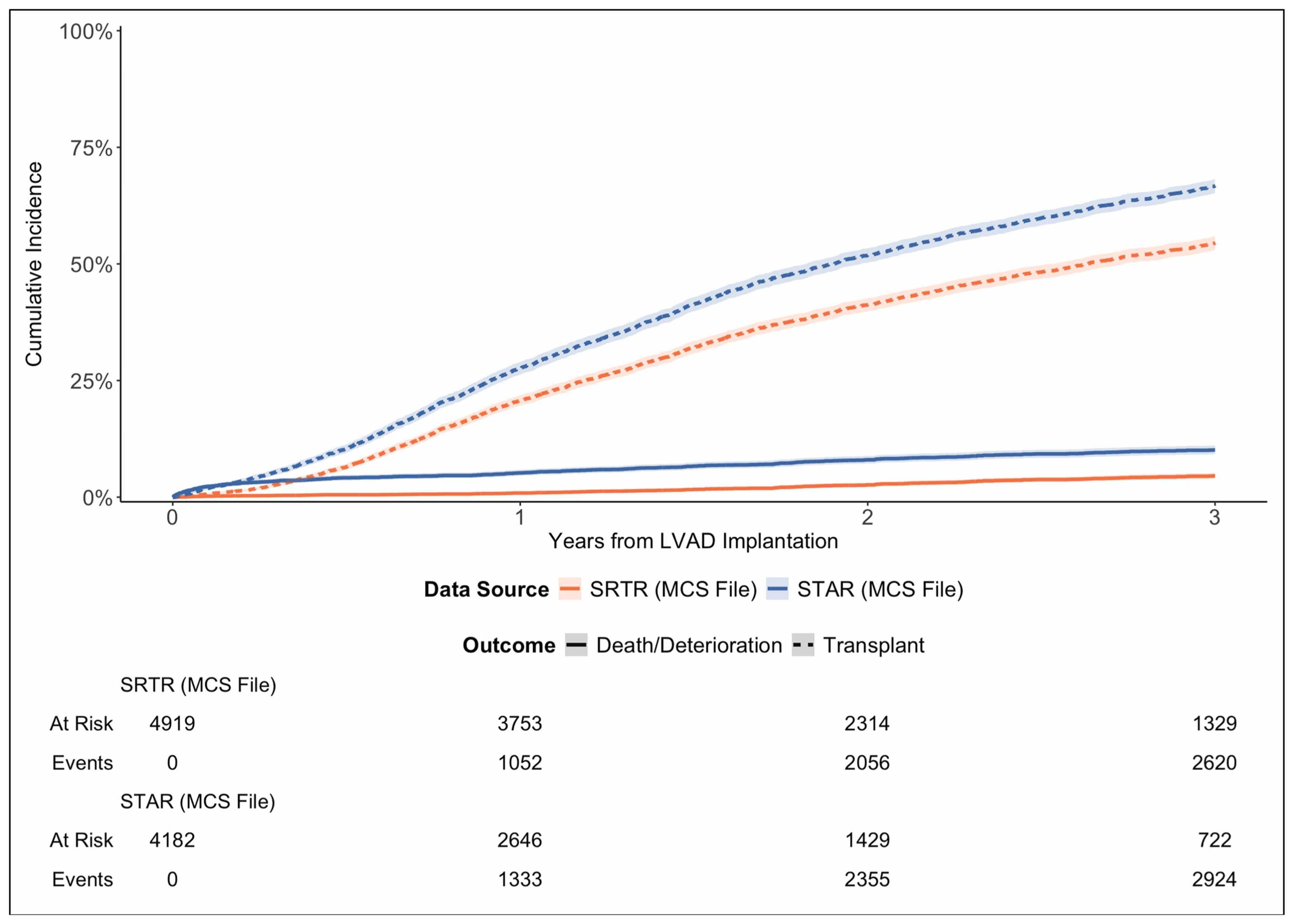

Artifactual Declines in Durable LVAD Utilization Among Heart Transplant Candidates: Selection Bias in Transplant Registries
The STAR MCS file excludes LVADs among currently listed candidates, producing artifactual declines in LVAD prevalence and incidence and inflated waitlist outcomes. Awareness of registry construction is essential for accurate interpretation of LVAD-related outcomes.
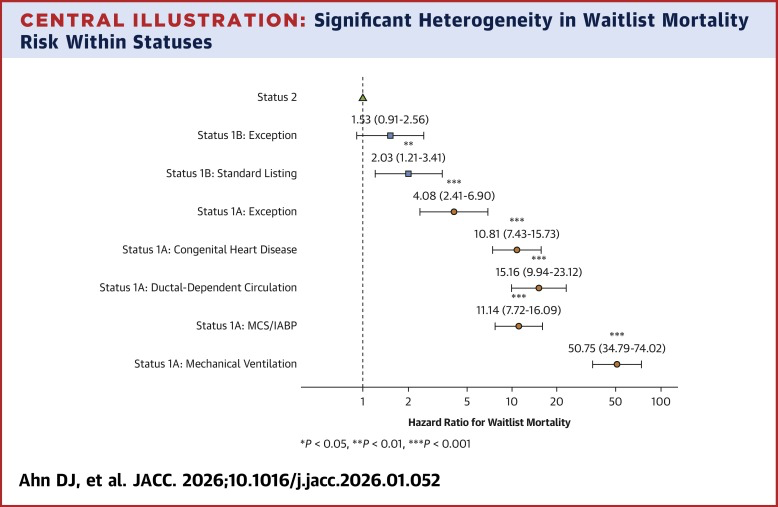
Status Exceptions and Misalignment of Medical Urgency in U.S. Pediatric Heart Transplantation
Pediatric heart transplant status exceptions are frequently granted to candidates who are not at the highest risk of waitlist death, contributing to misalignment between assigned medical urgency and actual mortality risk. The findings highlight opportunities to refine pediatric heart allocation policy.
Common Longitudinal ICU Data Format (CLIF)
The CLIF consortium establishes a common data standard for ICU data science, enabling privacy-preserving federated research across multiple hospital systems.
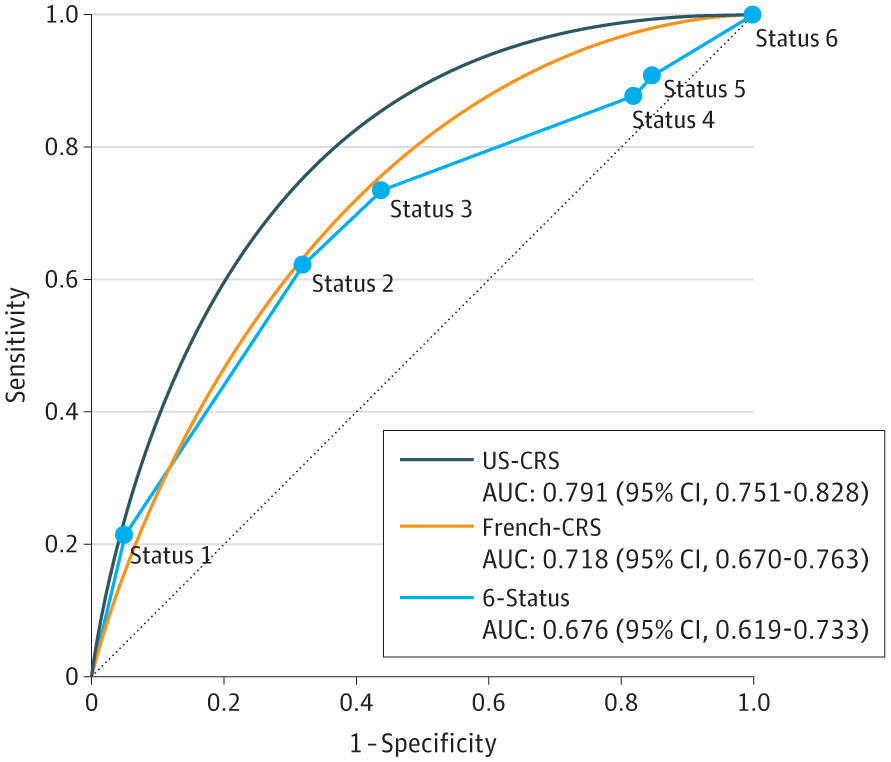
United States Candidate Risk Score (US-CRS) for Predicting Death Without Transplant in Adult Heart Transplant Candidates
A new risk score for heart transplant candidates predicts mortality on the waiting list, improving allocation beyond the current priority-tier system.
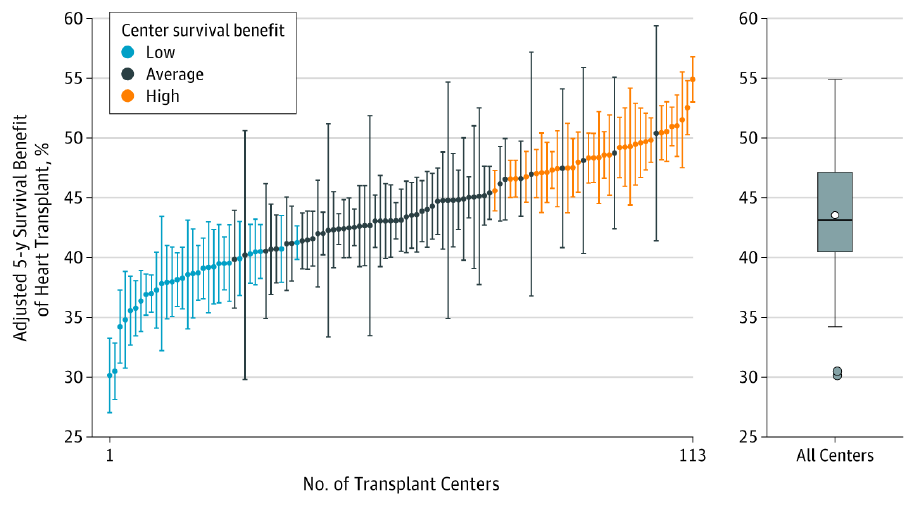
Association of Transplant Center With Survival Benefit Among Adults Undergoing Heart Transplant in the United States
The 5-year survival benefit associated with heart transplant varied across transplant centers, and high survival benefit centers performed heart transplant for patients with lower estimated waiting list survival without transplant.
Parker WF, Anderson AS, et al. JAMA. 2019;322(18):1789-1798.