
CLIF Consortium
The Common Longitudinal ICU data Format Consortium standardizes critical care data across 17 institutions and 46 hospitals to enable rapid, privacy-preserving multi-center research. Founded by Dr. Parker in 2023.
Funding
Our research is generously supported by:



Our Approach
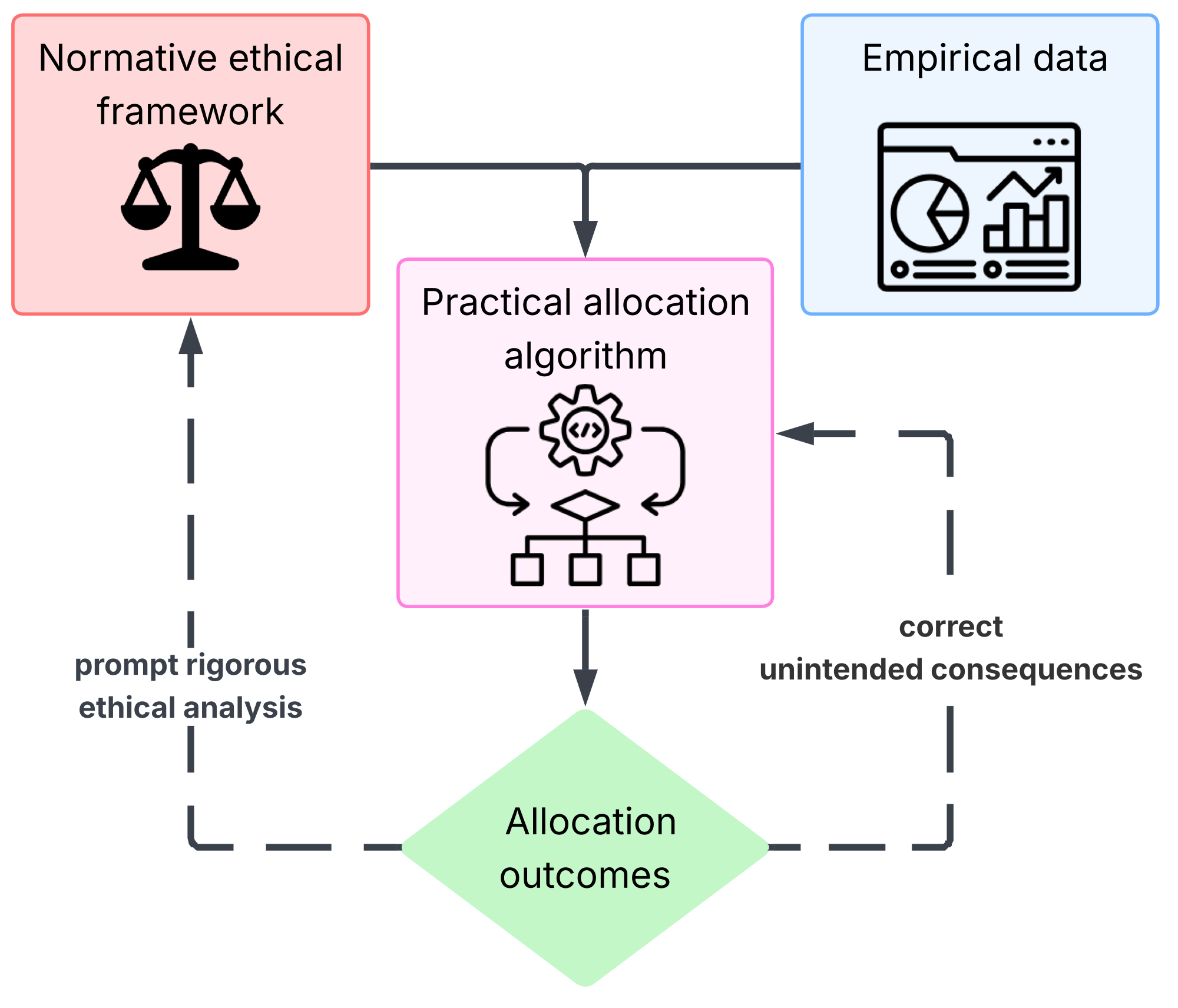
An integrated cycle of ethical analysis and empirical research.
“Although some are better than others, no single principle allocates interventions justly. Rather, morally relevant simple principles must be combined into multiprinciple allocation systems.”
— Persad, Wertheimer & Emanuel, The Lancet, 2009
The Parker HCA Lab is a quantitative bioethics lab, leveraging advanced data science methods and normative analysis to engage the wicked problem of the allocation of scarce healthcare resources. We believe both methods are equally important to generate satisfactory solutions.
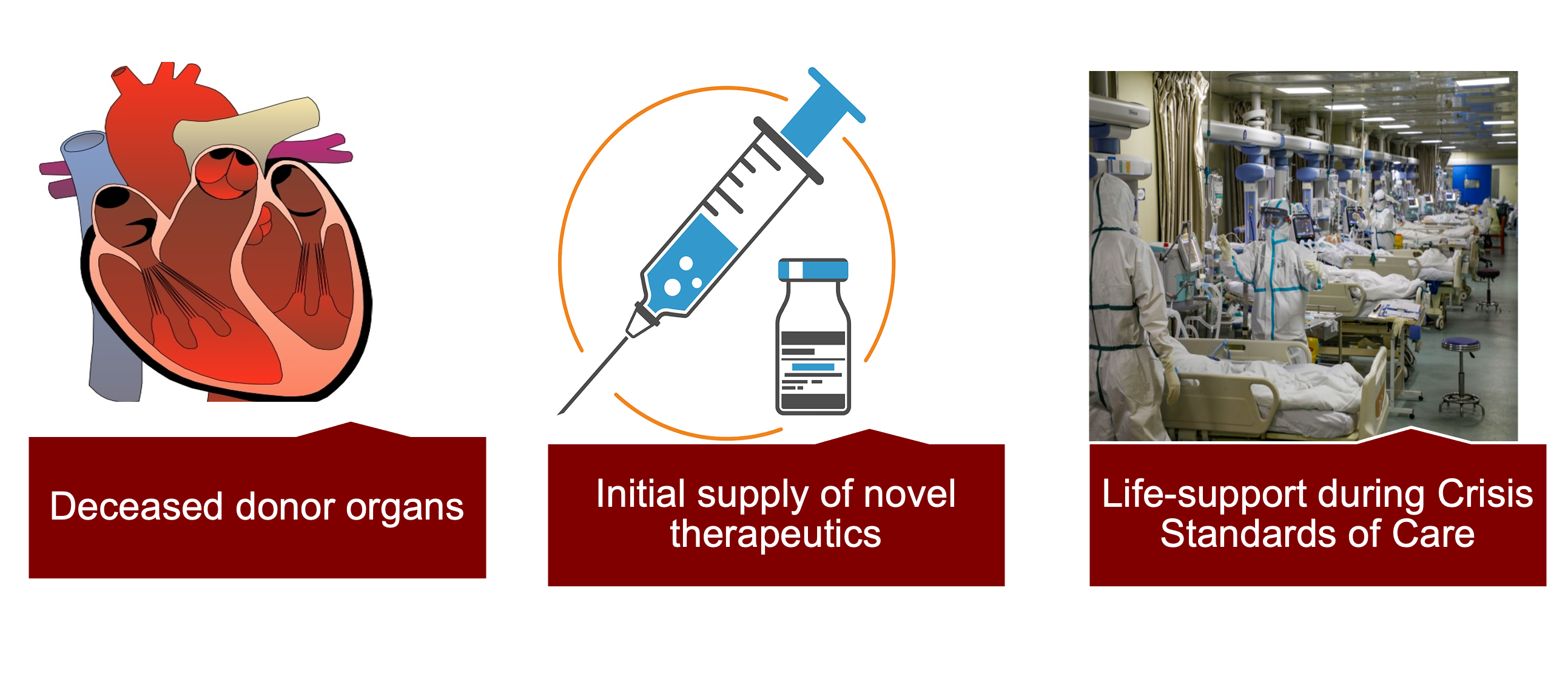
Research Areas
Our work spans three interconnected domains of scarce healthcare resource allocation.
Research Spotlights
Featured publications from the lab
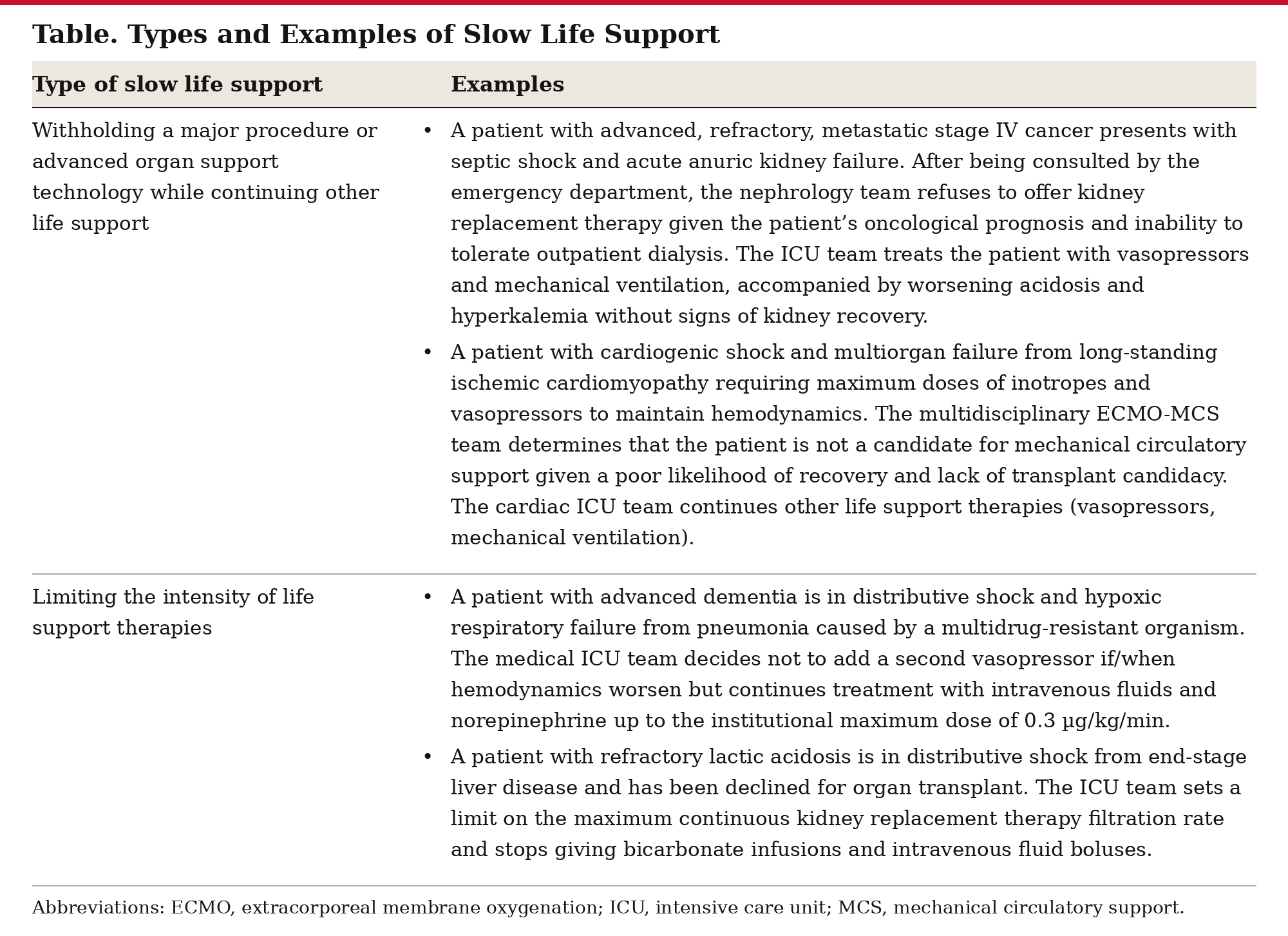

Slow Life Support for Imminently Dying Patients
Beyond communication, the boundaries of unilateral clinician authority must be clarified when initial shared decision-making is unable to negotiate a coherent life support plan. Informed assent, wherein clinicians explicitly disclose a recommended treatment path and its best-case and worst-case potential outcomes to patients or surrogates, may provide the most optimal balance of core ethical principles.
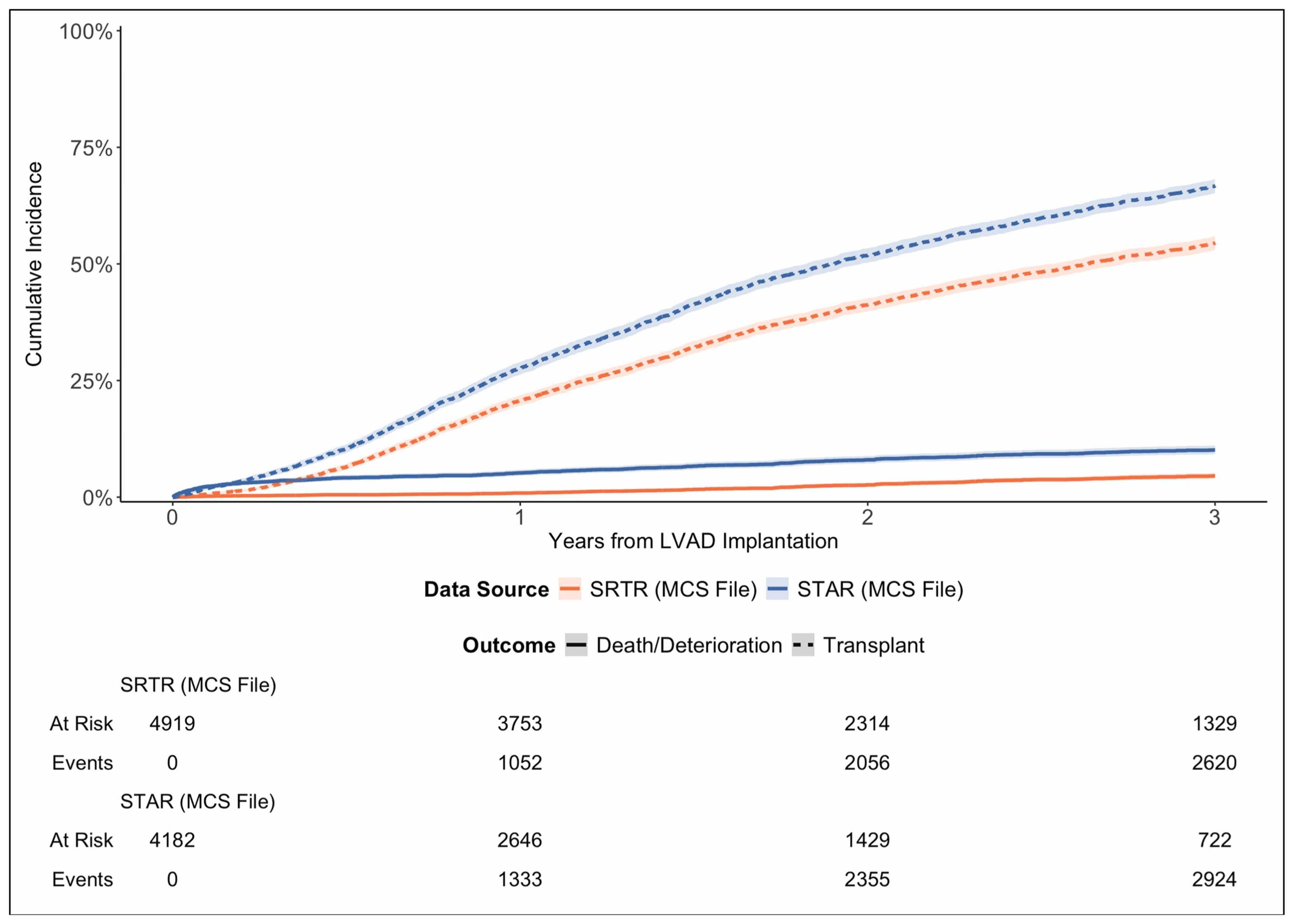

Artifactual Declines in Durable LVAD Utilization Among Heart Transplant Candidates: Selection Bias in Transplant Registries
The STAR MCS file excludes LVADs among currently listed candidates, producing artifactual declines in LVAD prevalence and incidence and inflated waitlist outcomes. Awareness of registry construction is essential for accurate interpretation of LVAD-related outcomes.
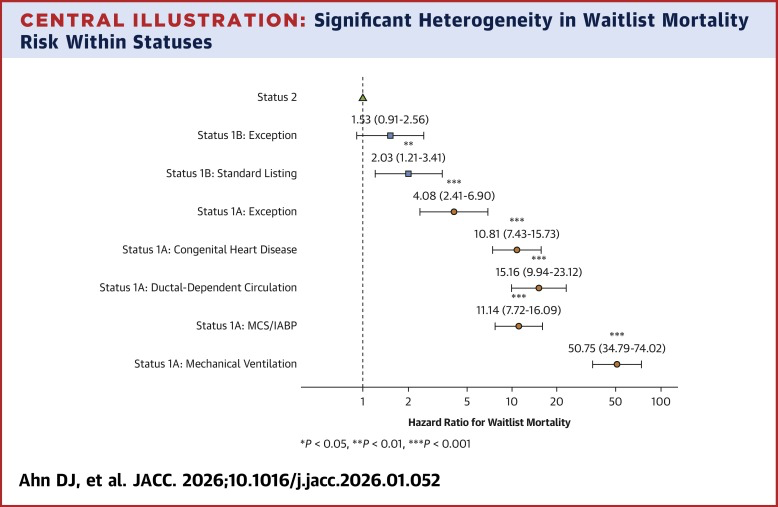
Status Exceptions and Misalignment of Medical Urgency in U.S. Pediatric Heart Transplantation
Pediatric heart transplant status exceptions are frequently granted to candidates who are not at the highest risk of waitlist death, contributing to misalignment between assigned medical urgency and actual mortality risk. The findings highlight opportunities to refine pediatric heart allocation policy.
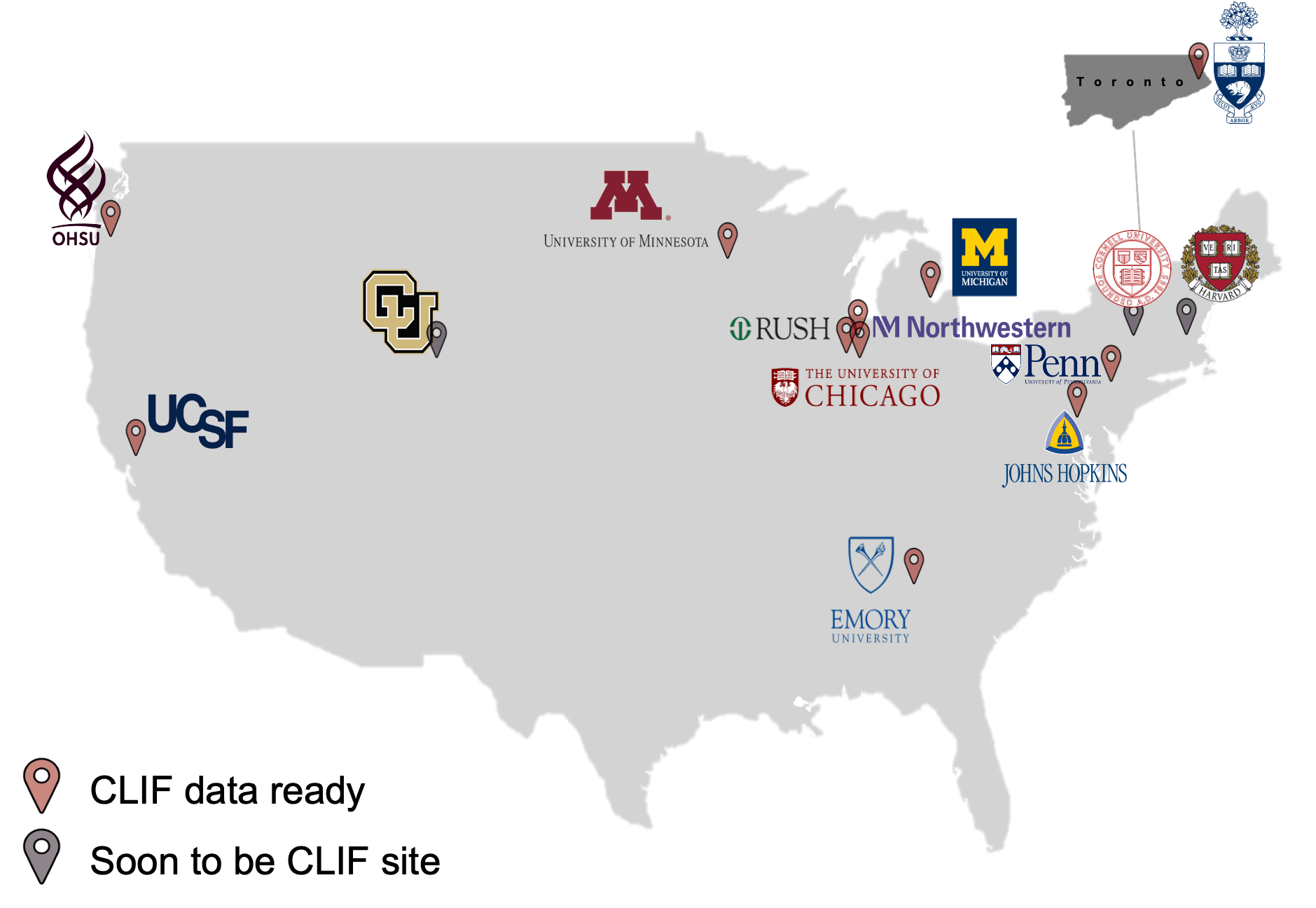
Common Longitudinal ICU Data Format (CLIF)
The CLIF consortium establishes a common data standard for ICU data science, enabling privacy-preserving federated research across multiple hospital systems.
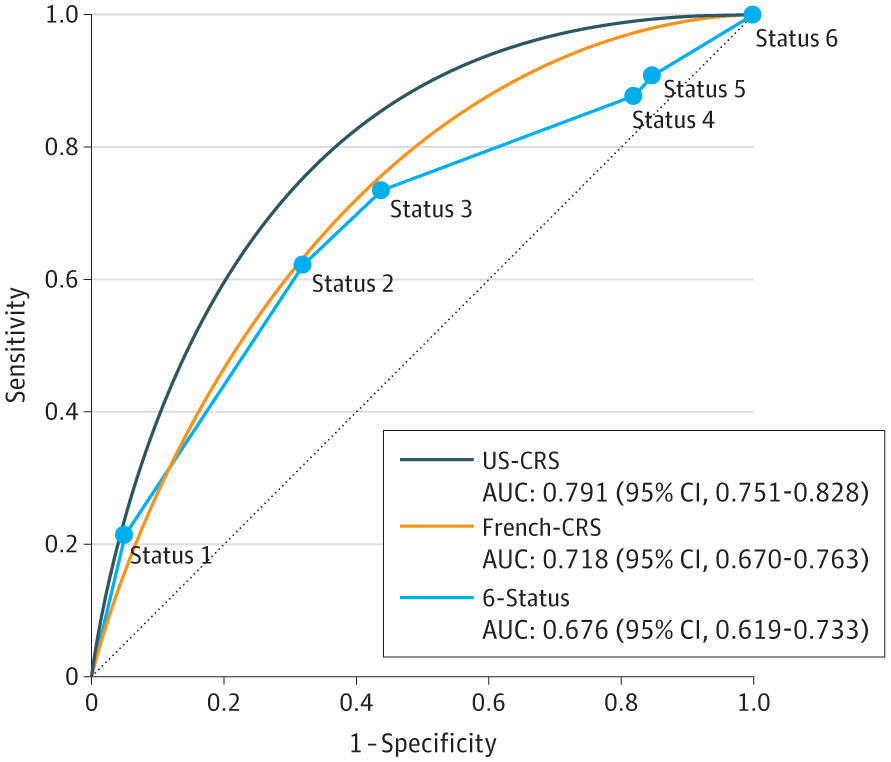
United States Candidate Risk Score (US-CRS) for Predicting Death Without Transplant in Adult Heart Transplant Candidates
A new risk score for heart transplant candidates predicts mortality on the waiting list, improving allocation beyond the current priority-tier system.
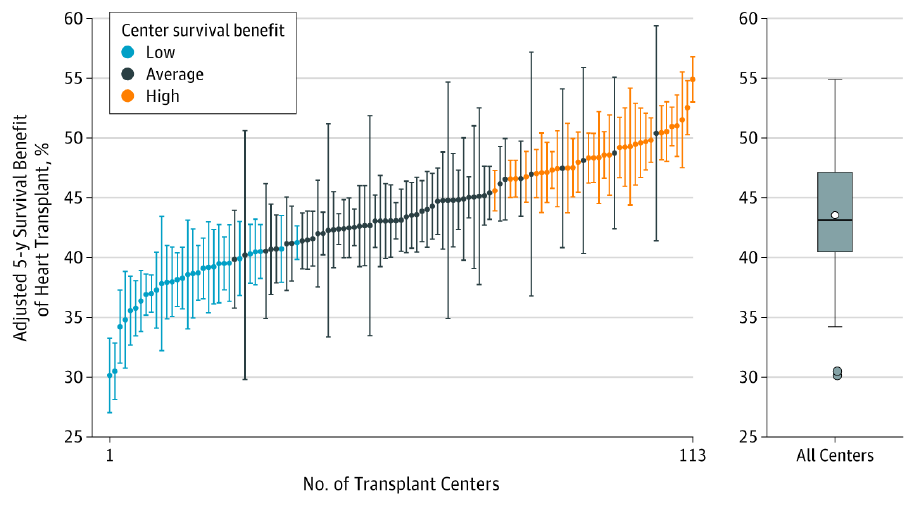
Association of Transplant Center With Survival Benefit Among Adults Undergoing Heart Transplant in the United States
The 5-year survival benefit associated with heart transplant varied across transplant centers, and high survival benefit centers performed heart transplant for patients with lower estimated waiting list survival without transplant.
Parker WF, Anderson AS, et al. JAMA. 2019;322(18):1789-1798.